What role does the hip joint play, human anatomy and the functions of this joint are questions that interest many people. One of the most important human abilities is walking. This human ability is achieved thanks to the unique structure of the hip joint, which consists of the acetabulum, located on the pelvic bone, and the head of the femur. This joint is similar in its anatomy and functions to the shoulder.
A distinctive feature is that the thigh is less mobile than the shoulder, and the main difference is that the hip joint must be a stable, powerful and more static support for the entire human body, since the lower limbs bear a greater load than the upper limbs. By the way, it is precisely thanks to this natural structure of this joint that it is much less susceptible to dislocations and other damage than the shoulder.
The main properties of the hip joint, with the help of which a person can walk, run, jump, and play sports:
- ability to move relative to different axes;
- support;
- flexion and extension;
- abduction and adduction;
- a whole range of hip rotational actions.
What is the structure of the hip joint
The main components of the hip joint in the human body are bone, muscle tissue and ligaments. The structure of the hip joint determines the large role of the cartilage tissue of the joint. Articular cartilage, which actually envelops the outside of the head of the femur and the acetabulum itself, is characterized by strength, smoothness and elasticity.
It is with the help of cartilage tissue that the soft sliding of bones occurs, as well as the distribution of the load on the bones during movement.
 The cartilage located in the hip joint acts like a porous sponge - when squeezed, articular fluid oozes out of it, and when weakened, the fluid again fills its porous structure. This liquid, which forms a protective film, is necessary to lubricate the surface of both the cartilage and the joint itself.
The cartilage located in the hip joint acts like a porous sponge - when squeezed, articular fluid oozes out of it, and when weakened, the fluid again fills its porous structure. This liquid, which forms a protective film, is necessary to lubricate the surface of both the cartilage and the joint itself.
The structure of the hip region also includes a capsule and ligaments. The hip joint is placed in a special strong capsule, which is attached to the pelvic bone with the support of the labrum at the back, and directly to the thigh itself at the front. In fact, the entire femoral neck is contained in this capsule.
As for the ligaments, the strongest of them in this section of the skeleton is the iliofemoral one, the main function of which is to prevent inward rotation and extension of the hip. The thickness of this ligament is up to 10 mm. This connecting part is necessary in the human structure to balance and hold the human body in an upright position.
The ischiofemoral ligament, located at the back, is no less important in the structure of the joint, since thanks to it, inward movement of the hip is anatomically impossible. This ligament arises from the ischium and runs upward. At the same time, the ischiofemoral ligament partially enters the articular capsule and connects to the trochanter of the femur itself.  Also placed in the articular sinus is a ligament of the femoral head, which consists of loose tissue.
Also placed in the articular sinus is a ligament of the femoral head, which consists of loose tissue.
The main purpose of this component of the hip joint is the connecting role; it provides a strong connection during movement. Along with this, in the plane of this ligament there are vessels directed to the head of the femur.
The pubofemoral ligament and the orbicularis ligament are equally important. The first is a bundle of fibers whose main function is to prevent abduction of the entire hip. But the circular arrangement of the second ligament corresponds to the rotational movements of the hip.
Characteristics of joint functioning
The physiological features of the structure of the hip joint in people directly affect health, endurance, well-being, and even gait. Due to its structure, the movements of the joint are very diverse.
The anatomy of the hip joint determines the maximum hip span, up to 122 degrees along the head of the femur or the frontal axis of the joint if the knee is flexed. Due to the tension of the iliofemoral ligament, extension in this department is up to 13 degrees. Rotation of the hip (adduction and abduction) around the sagittal axis with a straight leg is possible up to 45 degrees, but when the knee joint is bent, abduction is performed at 100 degrees.  Muscle tissue plays an important role in the coordinated functioning of the hip joint. In this section, the muscle tissue is quite massive, and it is designed to ensure the proper functioning of the joint. When moving (running, walking), muscles act as active shock absorbers.
Muscle tissue plays an important role in the coordinated functioning of the hip joint. In this section, the muscle tissue is quite massive, and it is designed to ensure the proper functioning of the joint. When moving (running, walking), muscles act as active shock absorbers.
Note that the most important muscles in this part of the body are the gluteal and thigh muscles, which need to be actively developed and trained. Reasonable load on the muscles of the buttocks and thighs is an excellent preventive measure that helps reduce the frequency and level of injuries.
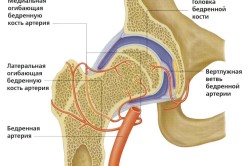
The blood supply to the hip joint occurs through the obturator and gluteal arteries; in the opposite direction, the blood passes through the iliac and deep veins of the department. Lymph enters this part of the body through the obturator canal, and outflow is carried out with the participation of the internal iliac lymph nodes.
Possible damage to the joint and causes of pain in it
The bones, muscles, ligaments of the hip joint and its other components must be protected and trained as much as possible. Often, for normal operation of this joint, you simply need to maintain a dynamic and healthy image life. However, even with this, both adults and children can feel discomfort and pain in the hip region.  The main factors of pain may be:
The main factors of pain may be:
- Injuries can be a variety of physical disorders of the capsule and ligaments, ruptures, fractures, bruises, muscle strains and other mechanical injuries.
- Separate features of the joint of each person. In this case, congenital pathologies and defects can have an impact.
- Diseases and injuries to other parts of the body. In such cases, the pain that overcomes another organ can “radiate” to the pelvic or thigh area.
- Systemic chronic diseases. This applies not only to diseases that are directly related to the joint (arthrosis, arthritis, tendonitis), but also to other diseases (for example, leukemia, tuberculosis, or infectious diseases).
Due to the heavy load on the hip joint throughout a person’s life, this section is often subject to various injuries. Most often, several types of injuries are diagnosed; for each of them, consultation and examination by a doctor are required!
Some of the damage:
- Injury. When bruised, the muscles in the joint area also suffer.
- Dislocation. A dislocation is a more serious injury that requires realignment of the joint.
- Femoral neck fracture. This injury is common in older people, but due to negligence and younger age you can get this damage.
Initial treatment of this injury requires traction and application of a plaster cast. If therapy is unsuccessful, the doctor may prescribe surgery (osteosynthesis).
Thus, the hip joint performs very important functions in the human body. In case of injuries, damage or diseases of this joint, you must consult a doctor for diagnosis and prescribing effective treatment.
The hip joint is the articulation of the femur with the socket of the pelvis. It is one of the largest in human body. Plays a vital role in movements and bears the load of the upper half of the body.
Unfortunately, pathology of the hip joint is a very common occurrence, especially in old age. Injuries lead to prolonged immobilization of a person and the development of severe complications.
The prerequisite for injury is the special structure of the joint, unusual blood supply, as well as the abundance of vulnerable elements.
Bone structures
What bones form a joint? Important formations are involved in creating the articulation: the head of the femur and the acetabulum of the bony pelvis.
The femoral head is a spherical structure that connects to the main part of the bone through a neck. Under these formations there are two outgrowths (trochanters). These are the ledges bone tissue, to which large muscles are attached, providing traction on the joint.
The acetabulum of the pelvis is an element that follows the contours of the femoral head, but with a larger diameter. Inside this fossa there is an articular surface that connects bone tissue with intra-articular cartilage.
Not a complete coincidence of the dimensions of the recess of the pelvis and the head determines the presence of auxiliary elements that give the structure strength and smooth movements.
Cartilaginous elements
The anatomy of the human hip joint is designed in such a way that intra-articular cartilage plays a significant role in movement. It is these structures that ensure perfectly smooth sliding of bones.
Cartilage provides trophism (nutrition), shock absorption, smoothes the force of movement, preventing stress on the bone.
The semilunar surface on the pelvic bone and the fossa of the femoral head are covered with cartilaginous layers.
The glenoid cavity is complemented by another structure – the acetabulum. This element is fixed around the acetabulum and makes it deeper, turning the lunate cavity into a large cavity accommodating the femoral head.
Fibrous structures
Maintain the components of the joints, limit excessive mobility, create a physiological correspondence between bone formations Fibrous connective tissue components - ligaments - help.
Intra-articular ligaments
A large bundle of fibers extending from the cartilaginous lip forms the transverse acetabulum ligament. Another fibrous element is attached to this structure and the surrounding bone tissue - this is the ligament of the head of the femur.
These fibrous structures are covered on the outside with synovial tissue, which nourishes the surrounding formations and ensures smooth gliding.
Extra-articular ligaments
The joints are surrounded by several strands of connective tissue that make up a fibrous membrane.
- The circular zone is a fibrous element with a transverse direction. It surrounds the femoral neck in the form of a loop and is attached to the bony pelvis under the acetabulum.
- The iliofemoral ligament is a wide structure with a thickness of 0.8–0.9 cm. It performs the most important function - it prevents hyperextension of the hip, and therefore keeps the body from falling onto the back.
- The ischiofemoral ligament is a much smaller fibrous element that limits excessive inward adduction of the limb.
- The pubofemoral ligament is a thin connective tissue cord on the inner part of the fibrous membrane. Prevents outward mobility.
This arrangement of fibrous fibers is necessary to perform the functions of articulation.
Joint capsule
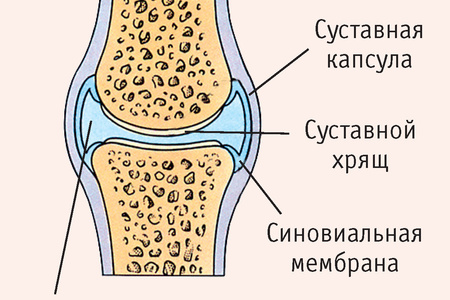
The special fibrous structure that forms the shell of the joint is the joint capsule. This wide cord originates on the pelvic bone around the circumference of the socket, and on the thigh below the head so that half of the neck remains under the capsule.
The structure of the capsule made of strong fibers is designed to hold the elements of the anatomical area together. The space inside the cavity is filled with synovial fluid, which performs a nutritional function and helps maintain smoothness.
Features of movements
The hip joint is a joint of bones that is shaped like a ball or bowl. This structure allows movements in the following axes: frontal, vertical and sagittal. Mobility is physiologically limited by large fibrous structures that form a thick membrane.
- In the frontal axis, flexion (120° in a bent knee) of the leg occurs, as well as extension, which is severely limited to 14°.
- In the sagittal plane, the leg is abducted and adducted in an amplitude of up to 90°.
- Around the vertical axis, the joint is capable of rotating movements up to 50° due to the anatomy of the femoral head. The volume is limited by intra-articular ligaments and large muscle elements of the femoral region.
Joint blood supply diagram
The structure of the vessels of the human hip joint explains the development of pathological mechanisms that occur during injuries. Therefore, it is worth understanding from what sources the joint is nourished:
From the deep artery of the femur (a large formation that feeds all the subcutaneous structures of this area), the internal and external arteries extending around the femur towards the joint.
From an important vessel that supplies the pelvic organs - the obturator artery - the acetabular branch, which carries oxygen and nutritional elements of the pelvic part of the joint, goes to the joint.
The gluteal branches, superior and inferior, depart from the internal iliac artery system. These vessels, through anastomoses (connections), participate in the nutrition of the joint.
The feeding circuit of the femoral head includes vessels from the periarticular plexus, which run around and inside the neck, providing blood supply to this structure. Therefore, with fractures of this anatomical region, starvation of the femoral head develops, leading to a disease such as avascular necrosis.
Clinical role of the joint

The human hip joint performs the functions of moving in space, forming posture, holding the body in the correct position, and others. Its entire anatomical scheme is aimed at creating a stable foundation for the torso on the one hand, and ensuring limb movements on the other.
These essential functions can be disrupted during the development of diseases such as:
- Fractures of the neck, acetabulum.
- Arthritis is inflammation of the joint.
- Arthrosis is the degeneration of bone and cartilage tissue.
- Cartilage injuries.
- Ligament ruptures and sprains.
- Rheumatic and systemic diseases.
The hip joint is one of the most important anatomical structures. It is important to take preventive measures and treat pathology in a timely manner.
These events must be trusted an experienced doctor. You should contact a specialist if the following symptoms occur:
- Pain.
- Crunching when moving.
- Clicking sensation.
- Swelling.
- Instability.
- Accumulation of blood in the cavity.
- Decreased mobility and smoothness of movements.
Timely initiation of therapy will improve the prognosis of any disease and preserve the correct anatomy of the most important human joint.
How to forget about joint pain?
- Joint pain limits your movements and full life...
- You are worried about discomfort, crunching and systematic pain...
- You may have tried a bunch of medications, creams and ointments...
- But judging by the fact that you are reading these lines, they did not help you much...
But orthopedist Sergei Bubnovsky claims that indeed effective remedy for joint pain exists!
Laboratory lesson
“The structure of the bones of the pelvic girdle and free lower limb”
The skeleton of the lower limb is divided into the skeleton of the lower limb girdle and the skeleton of the free lower limb.
The lower extremity girdle includes the pelvic bone, sacroiliac joint, and pelvic joints. The free lower limb is divided into the thigh, lower leg and foot. Its skeleton includes the femur, tibia and fibula, patella, hip, knee, tibiofibular, ankle joints, bones and joints of the foot.
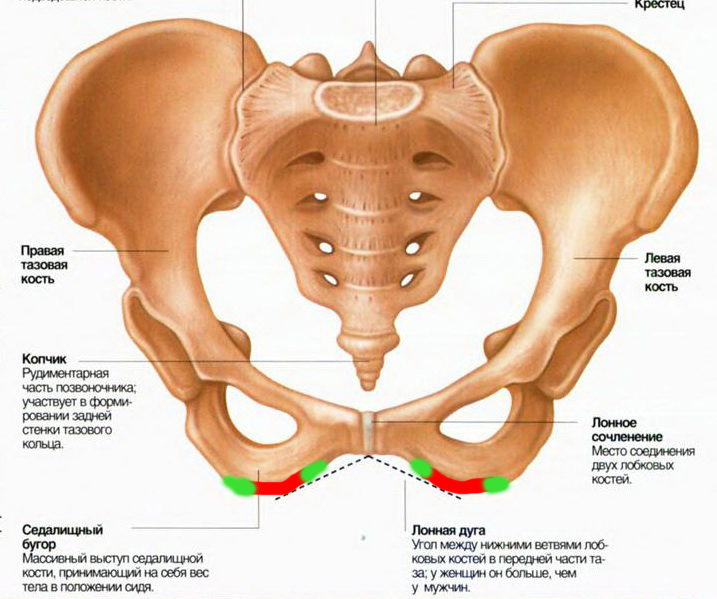
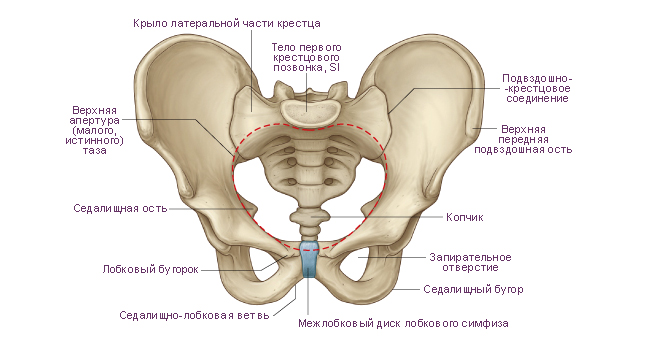
Hip bone refers to flat bones. At the back it connects to the sacrum, and at the front both pelvic bones are connected to each other by the pubic symphysis, forming the pelvis.
The three bones that make up the pelvic bone - the ilium, ischium and pubis - are involved in the formation of the acetabulum, which serves to connect the pelvis to the head of the femur. Each of these bones is formed as an independent bone, but by the age of 14-16 years or a little earlier they grow together.
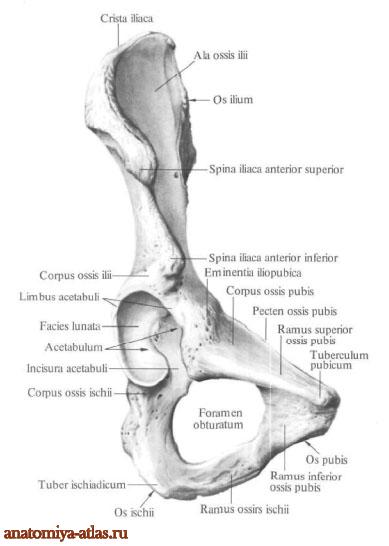
Ilium located above the acetabulum (Fig. 31). It has a thickened part - the body, which takes part in the formation of the acetabulum, and a wing, which is a wide, thin plate, thickened at the edges. Its upper edge is called the iliac crest. The abdominal muscles are attached to it. In front, the iliac crest ends in the superior anterior iliac spine, and slightly below it is the inferior anterior iliac spine. On the posterior edge of the ilium wing there are the posterior iliac spines - superior and inferior. They serve to attach muscles and ligaments.
Ischium has a body that continues into the branch of the ischium, connecting to the pubis. At the point where the ischium bends, a protrusion is formed - the ischial tuberosity. Above it is the ischial spine, which separates the greater sciatic notch from the lesser sciatic notch.
pubic bone consists of a body, as well as upper and lower branches. The body of the bone is involved in the formation of the acetabulum. The branches are located at an angle to each other and at the junction they form a symphysial surface for articulation with the pubic bone of the opposite side. Somewhat lateral to this surface is the pubic tubercle, from which the pubic crest extends, continuing into the arcuate line of the ilium.
The ischium, together with the pubis, limits the obturator foramen, covered by the obturator membrane.
Femur the largest long tubular bone. Its body is cylindrical and slightly curved forward. A rough line stretches along its back surface. On proximal epiphysis The femur contains its head, which bears the articular surface for articulation with the acetabulum. In the middle of the head there is a hole to which the ligament of the head of the femur, located inside the hip joint, is attached. The head is connected to the body of the bone by the neck, the axis of which is located at approximately 130° in relation to the longitudinal axis of the body of the femur. At the junction of the neck and the body there are two tubercles: bigAndsmall skewers. They are connected at the front intertrochanteric line, and behind - well expressed intertrochanteric ridge, which serve to attach muscles. Distal end The femur expands into two condyles - medial (larger) and lateral (smaller) - with an intercondylar fossa between them. Femoral condyles have articular surfaces for articulation with the tibia and the patella. The radius of the surface of the condyles (when viewed in profile) decreases posteriorly, which gives their outline the shape of a segment of a spiral. On the lateral surfaces of the femur, slightly above the articular surfaces of the condyles, there are protrusions - the medial plateau of the epicondyles, to which ligaments are attached. These protrusions, like the condyles, can be easily felt under the skin, especially if the lower leg is bent at the knee joint.
The strength of the femur is very high. When compressed along the longitudinal axis, it can withstand a load exceeding 1500 kg.
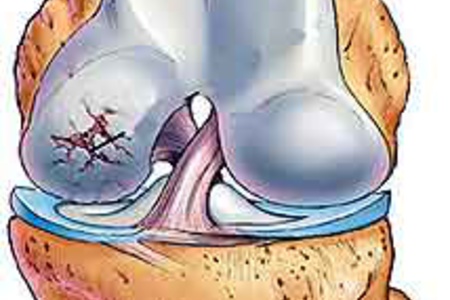
Patella located in front of the distal epiphysis of the femur. In shape, it somewhat resembles a biconvex lens with a blunter upper edge and tapering downwards. The patella is the largest sesamoid bone. It protects the joint from injury. With the help of a ligament, which is a continuation of the tendon of the quadriceps femoris muscle, the patella is attached to the tibial tuberosity.
Tibialbone located on the medial side of the leg (on the side of the big toe). Its proximal end is expanded and forms two condyles: medial and lateral. On the condyles on top there are articular surfaces that serve to connect with the femoral condyles, and between them there is an intercondylar eminence, to which the cruciate ligaments are fixed knee joint. The lateral condyle has an articular surface for articulation with the head of the fibula.
The body of the tibia is triangular in shape. It has three surfaces: medial, lateral and posterior. The medial surface is separated from the lateral by the anterior edge, which is easily palpable under the skin, like the entire medial surface of the tibia. The posterior and lateral surfaces are covered with muscles. The anterior edge at the top passes into the well-defined tuberosity of the tibia, which serves to attach the patellar ligament.
On the posterior surface there is a rough soleus muscle, to which it is attached. The distal epiphysis on the medial side has a protrusion directed downward - the medial malleolus, on the lateral side - a notch for connection with the fibula, and below - an articular surface for connection with the foot.
Fibula refers to long tubular bones. It is located laterally on the lower leg. Its proximal end ends in a head, which connects to the tibia, and the distal end forms the lateral malleolus. Both the head and lateral malleolus of the fibula can be easily felt under the skin. On the medial side of the lateral malleolus there is an articular surface that articulates with the talus. On the posterior surface there is a groove in which the peroneal tendons of the mouse lie.
Between the bones of the lower leg there is a gap covered by the interosseous membrane of the lower leg. Distally, the tibia becomes the foot.
Foot consists of three parts: tarsus, metatarsus and fingers. TO tarsal bones include: talus, calcaneal navicular, cuboid and three wedge-shaped - medial, intermediate and lateral (counting from the side of the big toe). They are all short spongy bones. TO metatarsal bones There are five short tubular metatarsal bones. The fingers consist of phalanges, which are also short tubular bones.
Talus located between the distal ends of the leg bones and the calcaneus, being a kind of bone meniscus between the bones of the leg and the bones of the foot. It has a body and a head.
On the upper surface of the body of the bone there is an articular surface in the form of a block, which serves to connect with the bones of the lower leg; on the anterior surface of the head there is an articular surface for connection with the scaphoid bone; on the body of the bone on the medial and lateral sides there are articular surfaces for connection with the ankles, and below - for connection with the heel bone.
Calcaneus makes up the posteroinferior part of the tarsus. This is the largest bone among all the bones of the foot. It distinguishes the body and the tubercle of the calcaneus protruding posteriorly. On the upper side, the bone has articular surfaces for connection with the talus, in front - with the cuboid bone, and on the medial side - a protrusion that supports the talus.
Scaphoid located at the medial edge of the foot, anterior to the talus, posterior to the sphenoid and medial to the cuboid bones. At its medial edge there is a tuberosity facing downwards, which can be easily felt under the skin and serves as a point for determining the height of the inner part of the longitudinal arch of the foot.
Cuboid located on the lateral edge of the foot and connects to the calcaneus, navicular, lateral cuneiform, 4th and 5th metatarsal bones. A groove runs along its lower surface, in which the tendon of the peroneus longus muscle lies.
Sphenoid bones- medial, intermediate and lateral - lie in front of the scaphoid bone, behind the first three metatarsal bones, medial to the cuboid bone. The wider part of the medial sphenoid bone faces down and the narrow part faces up, while the rest of the bones face the opposite way. These three bones, together with the cuboid bone and the bases of the metatarsal bones, take part in the formation of the arch of the foot, with the convex part facing upward and the concave part facing downwards.
Metatarsals. Each of the five metatarsal bones is tubular in shape. They distinguish between the base, body and head.
The bodies of the metatarsal bones are somewhat convex on the dorsum of the foot and concave on the plantar side. In their shape, these bones resemble triangular prisms. The longest bone is the 2nd, the shortest and thickest is the 1st. At the bases of the metatarsal bones there are articular surfaces that serve to connect with the tarsal bones, as well as with the adjacent metatarsal bones, and on their heads there are surfaces for connection with the proximal phalanges of the fingers. The 5th metatarsal bone has a protrusion along the lateral edge - a tuberosity, easily palpable under the skin. All metatarsal bones are easy to palpate on the dorsal side, since they are covered with a relatively thin layer of soft tissue; on the plantar side they lie deep under a large amount of muscle and subcutaneous fatty tissue. The metatarsal bones are not in the same plane, but form an arch in the transverse direction.
Finger bones. The toes are made up of phalanges. As on the hand, the first finger has two phalanges, and the rest have three. Often the two phalanges of the fifth finger grow together, and it has two phalanges. There are proximal, middle and distal phalanges. Their difference from the phalanges of the hand is that they are short, especially the distal ones. The foot, like the hand, has sesamoid bones. Here they are much better expressed and are located in the area of the connection of the first and fifth metatarsals with the proximal phalanges. Sesamoid bones increase the transverse arch of the metatarsus in its anterior section. There is also a sesamoid bone in the tendon of the peroneus longus muscle, located according to the groove on the lower surface of the cuboid bone. In addition, small sesamoid bones are sometimes found between the proximal and distal phalanges of the first finger.
During the evolutionary development of man, changes occurred in his skeleton, including the improvement of the structure of the pelvis. Walking upright led to a significant increase in the load on the pelvic bones. As a result, they acquired the appearance of a bowl with a wide base, which allowed the lower limbs to effectively perform functional activities.
The structure of the human pelvis is a rather complex anatomical structure that changes depending on age.
In children, the pelvic bones are connected to each other using elastic ligaments. In adulthood, the pliable connective tissue joint is replaced by bone tissue.
The relative position of the components of the hip joint also changes. Such transformations occur in order to withstand the load of a growing organism.
Gender features of the structure
The anatomy of the pelvic girdle depends on the gender of the person. This is due to the fact that women of fertile age are able to bear and give birth to children. It was labor activity that influenced the structure of the pelvis. Among the gender characteristics, the following should be highlighted:
- The transverse size of the pelvis in women significantly exceeds the longitudinal one. This wide shape provides support for the expanding uterus during pregnancy.
- For the physiological location of the amniotic sac, the bony base of the pelvis has a flattened bottom.
The parameters of the pelvic girdle are important for the normal course of labor, so they are measured in all pregnant women. The size and shape are assessed by a gynecologist using a special device - a pelvis meter. An additional measurement is performed intravaginally. Ultrasound allows you to accurately determine the internal dimensions of the pelvis.
European researchers have proposed using differences in the pelvic girdle in the fetus as a factor confirming the gender of the unborn child. Therefore, when conducting an ultrasound examination, the specialist pays attention not only to areas of ossification, but also measures key parameters of the pelvic bones.
Pelvic functions
The specific structure of the pelvic bones is determined by their functions. In the process of evolutionary development, man began to move vertically, which increased the load on the lower parts of the skeleton. In this regard, the bone base was strengthened, and the ligaments were replaced with strong joints. Among the main functions of the pelvis are:
- Support. The pelvic girdle bears the entire load of the upper half of the body.
- Motor. The lower limbs are attached to the pelvic bones, allowing movement in space.
- Maintaining balance. Due to changes in body position during development, a shift in the center of gravity occurred. The massive bones of the lower part of the body help stabilize it during various activities.
- Protective. The pelvic bones serve as protection for internal organs genitourinary and reproductive systems, lower digestive tract.
- Participation in labor. The anatomical features of a woman’s pelvis allow her to create physiological conditions for the growing fetus. Due to hormonal levels, changes in the ligamentous apparatus occur. This causes displacement of the bones during childbirth and further restoration of the pelvic girdle in the postpartum period.
Structure
The anatomy of the human pelvis has long been no secret. The structure of the skeleton of the lower limb has been fully studied. The development of instrumental diagnostic methods, such as X-ray examination, magnetic resonance and computed tomography, ultrasound, has made it possible to track the origin, formation and age-related characteristics of the pelvic girdle.
In some Internet sources, the skeleton of the lower extremities is mistakenly combined under the general name hip bone. We will look at how things really stand with the structure of the pelvis below.
Bony skeleton
The structure of the pelvis of a child and an adult is different. In childhood, the belt is represented by three bones connected by elastic ligaments. Between 14 and 16 years of age, the pliable connective tissue becomes calcified. There is a fusion of individual parts of the skeleton into one bone - the innominate. Let's take a closer look at each of them:
- Ilium. It is the posterior part of the pelvic girdle, connecting to the spine. It consists of a body and a wing ending in a crest. This structure serves as the attachment point for the muscular corset of the abdominal wall. There is a fossa on the inner surface of the ilium. She is famous for having right side The appendix is located in the body - part of the cecum, often involved in the inflammatory process.
- Ischium. It is located between the ilium and pubis and is represented by the body and the branch. On its surface there is a massive mound, which bears the main load when a person sits. In a vertical position, this anatomical formation is not visualized, since a thick layer of subcutaneous fat and muscle fibers are located above it.
- Pubic bone. The right and left pubic bones are connected to each other using cartilaginous tissue, forming the symphysis. Its role is great among women. During pregnancy, the properties of cartilage change. It becomes soft, which increases the distance between the pubic bones and expands the diameter of the birth canal. Above the symphysis there is a layer of fatty tissue that forms the pubis.
Hip joint

The pelvic girdle includes the hip joints, through which the lower limbs are attached. The junction of the ilium, ischium and pubis forms the acetabulum. It includes the articular part of the femur - the head. Thanks to the special shape of the surface, the hip joint is capable of movements in three planes, and the developed ligamentous apparatus prevents their excessive amplitude.
The articular part of the articulation is covered with hyaline cartilage. It ensures smooth sliding of the femoral head in the acetabulum. This is also facilitated by the synovial fluid filling the joint cavity. In addition to the lubricating function, it provides:
- cartilage nutrition;
- reduces the load, having a shock-absorbing effect.
The normal functioning of the hip joint guarantees a stable body position and ensures a full range of movements.
Vessels
The blood supply to the pelvic girdle is developed. It is provided by the large iliac artery, which divides into smaller branches. The capillary network entwines the internal organs, nourishes musculoskeletal system. The outflow of blood occurs into venous vessels located superficially or in depth.
Pathology
Pathology of the pelvic girdle is most often associated with traumatic exposure. The most dangerous are bone fractures that cause damage to internal organs. Violation of the integrity of the intestines and bladder significantly complicates the patient’s condition, worsening the prognosis for recovery.
Among diseases of the hip joint, a special place is occupied by dysplastic pathology associated with a congenital defect of the connective tissue of the joint. Modern methods diagnostics and treatment can effectively help patients, but in advanced cases the only way to help a person is endoprosthetics.
Os coxae, the steam room, in children consists of three separate bones: the ilium, the ischium and the pubis. In an adult, these three bones fuse into a single pelvic bone.
The bodies of these bones, connecting with each other, form the acetabulum on the outer surface of the pelvic bone. The ilium represents the upper part of the acetabulum, the ischium represents the posteroinferior part, and the pubis represents the anterioinferior part. During development, independent ossification points appear in each of these bones, so that until the age of 16-17 years, in the area of the acetabulum, the ilium, ischium and pubis are connected by cartilage. Subsequently, the cartilage ossifies and the boundaries between the bones are smoothed out.
Pelvic bone video
The acetabulum is limited by the thickened edge of the acetabulum, limbus acetabuli, which is interrupted in the anteroinferior part by the notch of the acetabulum, incisura acetabuli.
Inward from this edge, the inner surface of the acetabulum bears a smooth
articular lunate surface, facies lunata, which limits the acetabulum fossa, fossa acetabuli, located at the bottom of the acetabulum.
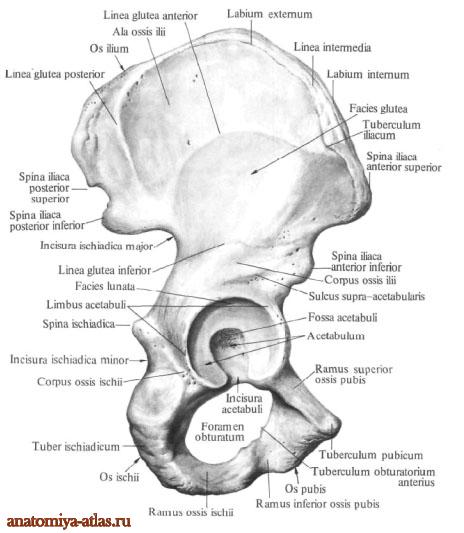
Ischium, os ischii, consists of two parts: the body of the ischium, corpus ossis ischii, and the angled branch of the ischium, ramus ossis ischii.
The body of the bone forms the posteroinferior part of the acetabulum. On the back surface of the body there is a bony protrusion - the ischial spine, spina ischiadica. Above and posterior to it is the greater sciatic notch, incisura ischiadica major, and below it is the lesser sciatic notch, incisura ischiadica minor.
On the anterior edge of the branch of the ischium, in the upper section, there is a posterior obturator tubercle, tuberculum obturatorium posterius. On the posteroinferior surface of the curved section of the branch there is a thickening with a rough surface - the ischial tubercle, tuber ischiadicum. The lower part of the branch in the anterior sections fuses with the lower branch of the pubic bone, ramus inferior ossis pubis.
pubic bone, os pubis, consists of three parts: the body and two branches - the superior branch of the pubic bone, ramus superior ossis pubis, and the inferior branch of the pubis, ramus inferior ossis pubis.
The body of the pubis, corpus ossis pubis, forms the anterior part of the acetabulum and directly passes into the superior branch, which runs forward, down and medially.
The upper edge of the superior branch is pointed and is called the crest of the pubis, pecten ossis pubis. In front, the ridge ends in the pubic tubercle, tuberculum pubicum. The lower edge of the upper branch is sharp and is called the obturator crest, crista obturatoria. The anterior end of this ridge forms the anterior obturator tubercle, tuberculum obturatorium anterius. Inwardly extending from it is the pubic crest, crista pubica, to which the rectus abdominis muscle is attached. The anterior section of the upper branch at an angle passes into the lower branch. On the medial surface of the superior branch there is a rough symphysial surface, facies symphysialis.